Euglycemic ketoacidosis is an urgent condition in which blood becomes excessively acidic due to high levels of ketones while blood glucose remains normal. Since ketoacidosis more commonly occurs alongside elevated blood glucose levels (hyperglycemia) due to insulin dysregulation, the normal levels of blood glucose seen in euglycemic ketoacidosis can hinder diagnosis and delay treatment. This article discusses the mechanism of euglycemic ketoacidosis to improve understanding, recognition, and intervention.
People with type 1 diabetes produce little to no insulin, which results in the inability of their cells to absorb glucose and shifts the body to a metabolic state called ketosis, characterized by the liver converting fat into ketones. Ketosis is generally safe and is not limited to those with diabetes; it is a common outcome of the low-carbohydrate ketogenic diet. During ketosis, insulin limits the extent of ketone production, as ketones are acidic, and keeps blood pH within a normal range, so those with type 1 diabetes who regularly take insulin typically do not develop ketoacidosis, a life-threatening condition in which the blood becomes acidic due to excess ketone production.
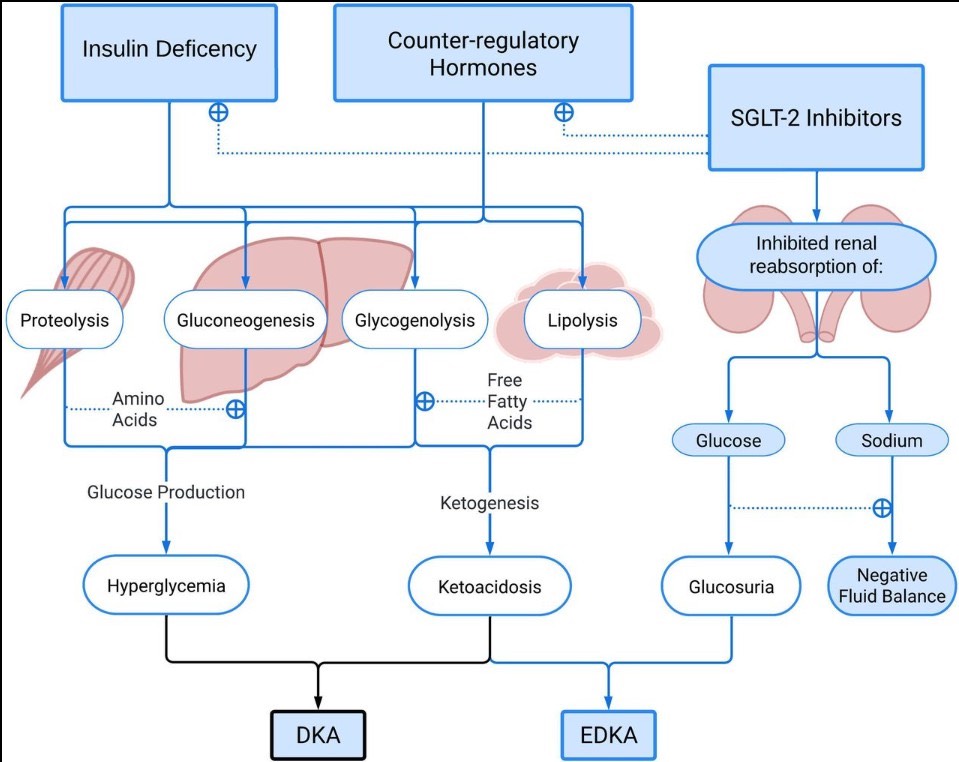
However, triggers such as infection, surgery, pregnancy, and pancreatitis can hinder insulin absorption, removing the check on ketone production and potentially leading to diabetic ketoacidosis (DKA).1 DKA is marked by ketoacidosis and simultaneous hyperglycemia, because in the absence of insulin or proper insulin function, glucose levels rise in the blood. DKA can thus be diagnosed in part by assessing a patient’s plasma glucose concentration.2
In rare instances, patients with type 1 diabetes (and, rarer still, those with type 2 diabetes), develop euglycemic diabetic ketoacidosis, in which ketoacidosis occurs alongside normal blood glucose concentrations, making it more difficult to diagnose. A mechanism that commonly causes euglycemic ketoacidosis is the inhibition of the SGLT2 protein through the use of inhibitors like dapagliflozin and empagliflozin.3
The SGLT2 protein in the kidneys normally promotes the reabsorption of glucose back into the blood. SGLT2 inhibitors instead cause the kidneys to excrete this excess glucose into urine.4 People with type 2 diabetes, and some with type 1 diabetes, take these inhibitors to manage blood sugar, but they can result in euglycemic ketoacidosis if triggers are present.
SGLT2 inhibitors are not the only cause of euglycemic ketoacidosis. Pregnancy, for example, is a possible cause, as one mechanism involves increased glucose intake by the fetus, which can result in a drop in the patient’s blood glucose level.5 Simultaneously, the body becomes more insulin-resistant during the latter stages of pregnancy, leading to an increased reliance on ketosis for energy. Additionally, parental plasma volume can increase up to 50% during pregnancy, leading to hemodilution and a subsequent drop in glucose concentration.
DKA is a significant cause of diabetes-related hospitalizations, and while euglycemic DKA comprises only about 3% of all DKA hospital admissions,6 knowing how to manage it is crucial. Because dehydration is common in this condition, as glucose excreted through the urine can pull water with it, care for this condition typically begins with the administration of fluids.1 Dextrose should be added to fluids in order to avoid low blood sugar and clear ketosis.1 Continuous insulin administration should follow.1 SGLT2 inhibitor use should be discontinued immediately after an euglycemic ketoacidosis diagnosis.1
With proper treatment, most patients make a full recovery from euglycemic ketoacidosis. However, delayed diagnosis and treatment can result in vomiting, persistent acidosis, and prolonged hospitalization. It is therefore critical that healthcare providers recognize the signs of euglycemic ketoacidosis early and promptly administer treatment.
References
1. Plewa, M. C., Bryant, M. & King-Thiele, R. Euglycemic Diabetic Ketoacidosis. in StatPearls (StatPearls Publishing, Treasure Island (FL), 2025).
2. Trachtenbarg, D. E. Diabetic ketoacidosis. Am Fam Physician 71, 1705–1714 (2005), PMID: 15887449
3. Chow, E., Clement, S. & Garg, R. Euglycemic diabetic ketoacidosis in the era of SGLT-2 inhibitors. BMJ Open Diabetes Res Care 11, e003666 (2023), DOI: 10.1136/bmjdrc-2023-003666
4. Padda, I. S., Mahtani, A. U. & Parmar, M. Sodium-Glucose Transport 2 (SGLT2) Inhibitors. in StatPearls (StatPearls Publishing, Treasure Island (FL), 2025).
5. Algaly, G., Abdelrahman, A. & Ahmed, S. M. I. Euglycemic diabetic ketoacidosis in a pregnant woman. J Am Coll Emerg Physicians Open 4, e13089 (2023), doi: 10.1002/emp2.13089
6. Yu, X., Zhang, S. & Zhang, L. Newer Perspectives of Mechanisms for Euglycemic Diabetic Ketoacidosis. Int J Endocrinol 2018, 7074868 (2018), DOI: 10.1155/2018/7074868